
Suffer from Migraine Auras? It’s in Your Brain, Not Your Eyes
Indu Shanmugam had planned to pull an all-nighter at her college library. But a slight headache and tiredness made it challenging to think, so she decided to cut the study session short and head home.
A commuter student, Shanmugam began the 40-minute drive back to her parents’ house from Concordia University in Portland, Oregon. Next thing she knew, she was being stopped by the police for erratic driving.
That was 16 years ago, when Shanmugam was 26. She didn’t realize it, but she was experiencing her first migraine aura.
Shanmugam remembers starting to feel queasy while driving. Her headache became much worse. She apparently was swerving a bit, and she knows she missed her exit. She saw the police car’s flashing lights behind her, so she moved over and stopped on the righthand side of the road to allow the vehicle to pass. She didn’t realize she was the one being pulled over until the police car turned into the lane behind her.
After the police approached her driver’s door, Shanmugam vomited all over her dashboard. She became dizzy, and her vision blurred, with funny shapes appearing in her periphery. She told the officers she didn’t feel well.
“The cops probably thought I was a college student partying all night, which is not what happened,” she said. After she passed a breathalyzer test, the officers realized she might be having a medical episode and called for an ambulance.
At the hospital, the doctors ruled out stroke and confirmed there were no drugs in her system. “And that’s how I found out I had migraines,” she said.
Specifically, Shanmugam gets migraine auras. Migraine auras are a type of migraine that affects vision. They can occur with or without a headache. Migraine auras can also cause sensory disturbances—like tingling, numbness and weakness—and sometimes cause difficulty speaking. Because impaired speech, weakness and some of the other symptoms are also symptoms of a stroke, it’s important to seek medical attention quickly if they happen.
What Are Migraine Auras?
You may hear these called “ocular migraines” or “eye migraines,” but those are not accurate medical terms. You may also hear about “retinal migraines,” which are something entirely different and more rare.
The accurate term is “migraine aura” or “migraine with aura.” You may also hear about “visual aura,” a medical term to describe the symptoms affecting the eyes during migraine aura.
Migraines affect about 12% of the U.S. population, according to the Cleveland Clinic. Women are three times more likely to have migraines than men are, and migraines tend to be genetic, meaning they run in families. About 25% of people who have migraines experience aura.
While much of what is happening during a migraine aura affects what a person can or cannot see, the problem is coming from the brain, not the eyes.
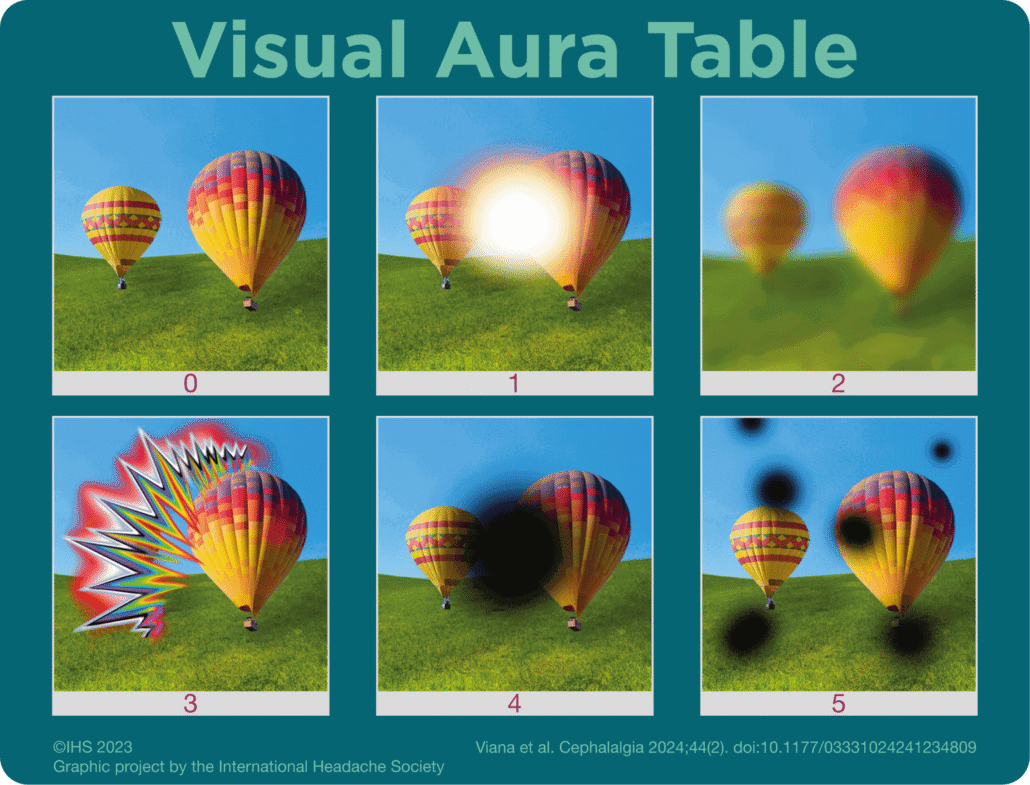
For most people, a migraine aura causes “scintillating scotoma,” which usually appears as a zigzag or shimmering pattern that moves across their vision, explained Deborah Friedman, MD, MPH, a headache medicine specialist and neuro-ophthalmologist who is owner of the Yellow Rose Headache and Neuro-Ophthalmology practice in Texas.
Here’s how Dr. Friedman described it: “Usually people will notice that there’s something amiss just off to the side of their vision. Over time, it starts to enlarge, and it takes on a zigzag shape. It’s semi-circular and starts to move and expand over the visual field.”
The aura can be seen with both eyes open, one eye open, or both eyes closed—because, remember, it’s coming from the brain, not the eyes.
“The shimmery part can either be in black and silver, or sometimes it’s in color. Often, within this border, there’s an area that’s dark that people can’t see through. That’s the ‘scotoma.’ The flashing is the ‘scintillation,’” Dr. Friedman said.
This strange vision gradually gets bigger and moves across your visual field. Then, it breaks up into pieces and goes away.
Because people are “seeing” migraine auras with their eyes, they may explain that it is starting in their left or right eye and moving across to the other side.
However, both eyes are involved, said Benjamin Frishberg, MD, a headache medicine specialist and neurologist specializing in neuro-ophthalmology at the Neurology Center of Southern California. “When it’s off to one side, people often think that it’s in one eye. Often, people say, ‘It’s in my left eye.’ And I have to ask, ‘What happens when you close your eyes?’
“With migraine aura, when you close your eyes, you still see it,” Dr. Frishberg continued. “Migraine aura can occur in people who are blind—especially people with acquired blindness—because it is a brain condition, not a vision or eye condition.”
A migraine aura can last 5 to 60 minutes, but for most people, it lasts about 10 to 25 minutes. If a person also experiences a headache, it typically starts after the aura. For many people, the headache then builds in intensity into a migraine, Dr. Friedman said.
While it’s unclear why some people get migraine auras, what is happening in the brain during an aura is a bit more clear. It’s likely caused by “cortical spreading depression” in the brain. This is a complex process, and scientists aren’t exactly sure why it happens.
For some reason, a rapid change in brain cells occurs that then causes a wave of electrical activity to develop and spread in the brain. That is what causes the shapes and shimmers to move across your vision. Think of a it as a power surge in your brain—followed by a dimming of the lights.
“It moves in such a way that it correlates with the time it takes to cross the cerebral cortex, which is about 20 minutes,” Dr. Frishberg said.
How to Prevent and Treat Migraines
Shanmugam is now 42 and lives in Lowell, Massachusetts. She doesn’t get as many migraines now as she once did, thanks to finding the right mix of medications and avoiding triggers.
And like most people with migraine auras, she can tell when a migraine is coming on. This alert system means it’s safe for most people with migraine auras to drive, allowing them time to pull over safely before the aura starts, Dr. Frishberg said.
Before an aura starts, “I get very nauseous,” Shanmugam said. “And then I feel a tingly feeling on one side of my body, and then my vision changes, like I’ll see a shape or aura.” When that happens, she immediately takes Imitrex (sumatriptan) to lessen or stop the migraine.
Nexplanon (etonogestrel), a hormone-releasing birth control implant in her arm, has helped level out her hormones, reducing the number of migraines. She also takes a magnesium supplement, under a physician’s care. Over the years she has figured out triggers to avoid, like dehydration and nitrates in foods like deli meat.
The triggers—or what causes a migraine to develop—are different for each person. Keeping a migraine diary of what you did in the hours before the migraine can offer clues. Track potential triggers like stress, dehydration, types of food, weather or altitude changes, and too much or too little sleep.
“People with migraine do best if they have an environment that doesn’t change much: Get up and go to bed at the same time. Don’t skip meals. Try to have a good homeostasis—staying kind of level and not doing too much one way or the other can help,” Dr. Frishberg said.
Some people’s migraines may be triggered by flashing lights or strobe effects—like when you’re driving down a tree-lined road and row after row of trees pass by your peripheral vision quickly.
A glint off a window or shiny car on a sunny day might be a trigger for some. Dr. Frishberg had a patient who lived next to a body of water and would get migraines when they looked at the way the light sparkled on the water as the sun set.
Medicines that treat migraines include a class of drugs called “triptans”—this includes the sumatriptan that Shanmugam takes. Triptans do not prevent migraines. Instead, patients take the medicine when a migraine is coming on, and it blocks serotonin and calcitonin gene-related peptide (CGRP), which is a neurotransmitter in the body that can trigger migraines. This “blocking” constricts blood vessels and decreases inflammation, which can reduce painful symptoms.
Newer Drugs: CGRPs
A newer class of drugs is the CGRP antagonists. The first CGRP antagonist was approved in 2018 by the U.S. Food and Drug Administration (FDA). They are currently only available as brand-name drugs, not generics.
CGRP antagonists work by blocking CGRP. Studies have shown that people with migraines have higher levels of CGRP in their body, according to GoodRx. Because of this, CGRPs can prevent, as well as treat, migraines in some people.
There are three CGRP antagonists taken as pills to treat a migraine attack. A fourth is a nasal spray to treat the migraine quickly. These type of CGRPs are also called “gepants.”
Another type of CGRP-targeting medication are monoclonal antibodies, or CGRP mAbs. These are intended to prevent migraines. There are three CGRP mAbs available, given as injections either monthly or every three months. A fourth is given as an IV infusion every three months.
The American Headache Society changed its guidelines in 2024 to recognize that CGRPs can now be first-line treatment for migraine sufferers. Previous guidelines recommended trying triptans and other medications first and prescribing CGRPs only as a last resort. But more studies and more clinical expertise—meaning more years of doctors treating patients with CGRPs to see how they respond—have shown how well CGRPs work, according to the American Headache Society.
Botox injections also prevent migraines in some people. Botox works by blocking pain signals and is approved by the FDA for adults who have 15 or more migraines a month.
Seeking out a migraine specialist can help you find the right treatments for you. It may take a bit of trial-and-error to discover triggers to avoid and medications that work for you, but more treatments are available today than just a few years ago.





