
What to consider after a loved one receives a diagnosis of dementia
The patients and families in my clinic are often referred to me for this key question: “Do I have dementia?”
Family members may sense that something has changed for their loved one. Patients may know something is different but may not be fully aware of the problems and changes they are experiencing. This can lead to a great deal of fear around the potential diagnosis and what the future may hold after that diagnosis. It also highlights the importance of thorough evaluation and clear communication around assessment findings. Dementia is a familiar term to most people, even though it is often used incorrectly. The word, “dementia,” refers to the depth and breadth of cognitive and practical problems. However, the term “dementia” does not speak to what is causing those problems. The underlying cause of dementia can be any number of things, including Alzheimer’s, Parkinson’s, stroke, and many more. Despite the cause, informing someone that they have signs of dementia—of any kind—is often heartbreaking news for patients and their families. It’s also difficult for the doctors who deliver that news. This is why many doctors hesitate to share the diagnosis or defer the responsibility to specialists.
This is where I come in as a neuropsychologist. Breaking that news is one of the single most difficult things that I do in my clinic, and yet I do it often. In helping patients and families digest this news, I’ve come to see it as an honor to walk patients and families through the practical first steps of being introduced to the realities of the diagnosis.
To help make this happen, I ask families to prepare for the worst-case scenario and live for the best case.
I encourage families to prepare for problems ahead of time instead of responding when the problems are too big to ignore. Emotions can take over and cloud judgment too much in those times. First, I ask families to think through their loved one’s practical needs. How much practical trouble is the patient having in their day-to-day life? What help do they need now? How can they prepare for, if, or when that trouble gets worse? I ask them to be familiar with their loved one’s daily routine and their usual needs. A big part of this is familiarizing themselves with their loved one’s medication regimen and financial situation. It’s ideal if families can be comfortable with these needs before their loved one needs help, but it’s never too late to start.
I also ask families to update their home emergency plan, to make sure their loved one is safe in case of a house fire or natural disaster, for instance. These situations can be doubly hard for a person with any kind of cognitive problem.
Some of the questions to think about are harder. I ask them to think long and hard about driving—how much longer can the person who has received a dementia diagnosis keep driving safely? The answer is different for every person. The gold-standard driving skills test is a practical behind-the-wheel test with an occupational therapist who is specially trained to examine driving skills. Neuropsychological evaluation can also assess some skills that are important to driving, such as how fast the brain can process information and how easy it is to juggle attention. Sometimes, scaling back driving to good weather conditions, within a few miles from home, with little to no distraction in the car might be the most appropriate choice, and sometimes, no driving altogether is the better option.
I ask families to consider their plans for their loved one’s long-term care. When will they need to ask for help in caring for their loved one? What might that help look like? For different families, and at different times for the same family, it might mean help from friends and neighbors, scheduled respite care from a professional caregiver, live-in help, or nursing home placement. Considering all options ahead of time can be a great comfort when and if a patient needs more hands-on care than their loved ones can give alone. The financial aspect is also important to consider. Do they have insurance policies or benefits for long-term care? They may also want to contact an expert in elder law for advice on how to protect their loved one’s assets if their condition worsens and long-term nursing facility care is needed.
I ask families to make sure that their loved one has Advance Directives for Health Care (this is also known as a Living Will) and Power of Attorney for health care, legal decisions, and finances. Many states, including my home state of Kentucky, have premade documents to cover the basics of a living will and health care power of attorney. Families should be aware that power of attorney for health care does not apply to finances and legal issues, so asking a trusted attorney for guidance on those issues can be important. Once the documents are done, keeping multiple copies of them in a safe place with other important papers, as well as on file at the patient’s primary doctor’s office, can give a lot of peace of mind.
Beyond these important issues, I ask loved ones to think about what I call The Big 5. These are five key parts of brain health for anyone and need special attention for families dealing with a diagnosis like dementia. (Click here to download a PDF of the infographic below.)
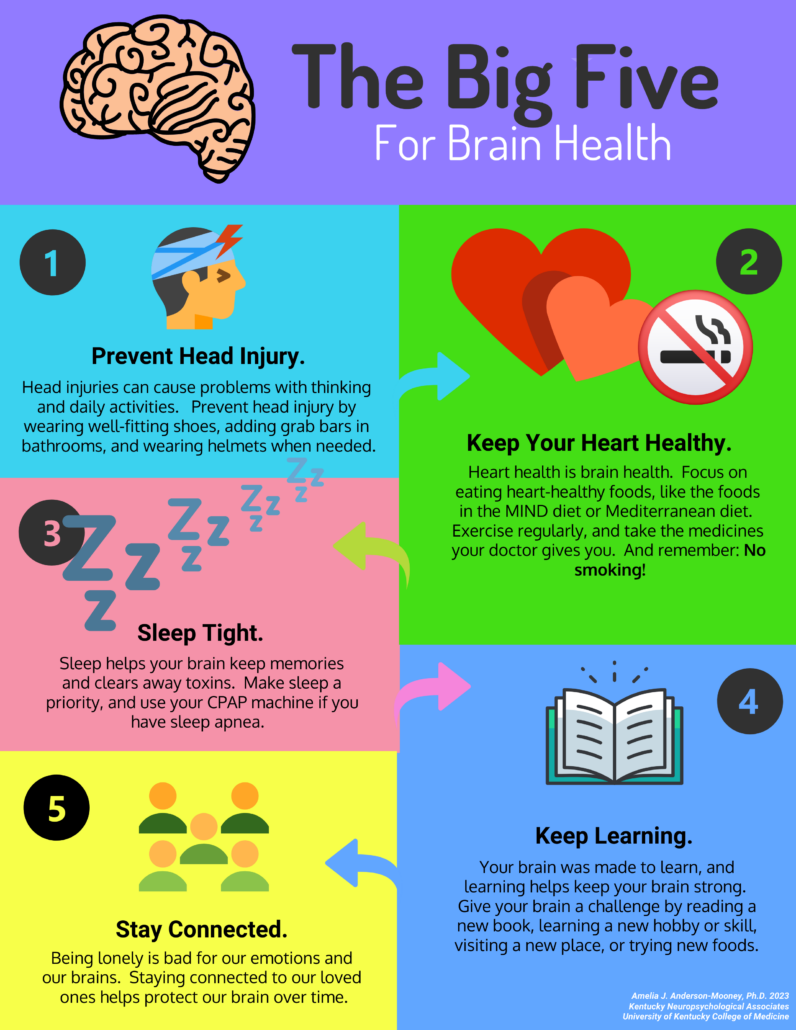
Head injury prevention
Falls are bad for older adults in just about any condition; for those with dementia, they can speed up the onset. When elders fall and hit their heads, it can cause bleeding on the brain. I advise family members of my patients to always protect the patient’s head. This can be as simple as making sure pathways are clear and shoes fit well. Be aware of little pets that love to be underfoot. Put bars in the bathroom and on the stairs. Make sure area rugs don’t curl up and cause hazards. Sometimes, an Occupational Therapist can do an in-home evaluation to give pointers for safety.
Heart health
In general: Anything that’s good for your heart is good for your brain. Your heart is pumping about 20 percent of your blood straight to your brain every time your heart beats—a large closed-loop system of pipes connects them. If something goes wrong with a patient’s heart, it increases the chances that something can go wrong upstream in the brain. This means it’s important to stay on top of things like blood pressure and sleep apnea. It also means following a heart healthy diet, like the MIND diet, avoiding processed foods, and getting reasonable, regular exercise. One of the most important keys to heart health is well-known: No smoking! Quitting smoking, or never starting, is one of the single most important things we can do for our brain health and for the rest of our bodies.
Sleep
I tell my patients to treat sleep like it is sacred. When we sleep, our brains go through their regularly scheduled maintenance programs. It’s like taking your car in for an oil change and transmission service —especially during REM sleep and deep sleep. We all need this sleep, but people with dementia might need it even more. Some new research says that deep sleep might help slow down the progress of the disease. This shows why sleep apnea can be such a problem. Sleep apnea disturbs our sleep cycles, sometime keeping us from getting enough REM and deep sleep. It also rations the oxygen in our brains, which can make thinking problems worse. Sleep apnea can also increase the chances of heart attack and stroke, which can damage the brain even more. If you have sleep apnea, good treatment is important.
Cognitive activity
Especially as we age, we must keep thinking and using our brains. Our brains are made to learn, especially in the real world, engaging in the activities of real life. Read the book. Visit a new place. Try a new food. Learn a new hobby. Meet some new people. Our brains love all that stuff. Sudoku and crossword puzzles are great, so long as they are engaging for someone’s brain.
Stay Connected
There are all kinds of research proving that loneliness is toxic to our physical bodies. Isolation is not good for us. I always tell loved ones and family members of my patients: Now is the time to double down on relationship. Check in on them, make sure they have every opportunity to connect with friends and family to maintain their important relationships and connections. This is especially important if a patient cannot drive: Those folks too often get cut off from the outside world. While doing this, it’s also important to make sure the patient doesn’t get overwhelmed. Because of this, families might need to rethink how best to offer those connections. They might need to rethink how to manage family traditions, like big holiday dinners. Again, talking about these issues ahead of time can help immensely.
Remember when I said that I want my patients to live joyfully, no matter their diagnosis? I know none of this sounds all that joyful. But remember, I want to help these families prepare for the worst and live for the best. Because of this, I also ask them to go have fun. Especially if the diagnosis comes early, I tell them: Take the trip, do the experience, get after it. If there is anything you’ve dreamed about doing, do it. Spend time together and love one another with intention and dedication. Do this, and some of your best memories may be ahead of you, not behind you.
Click here to download a PDF of The Big 5 infographic.
For more information about elder law, check out the National Elder Law Foundation and the National Academy of Elder Law Attorneys.







