What is a stroke?
If cardiac arrest is sometimes called a “heart attack,” it makes sense that nurses and doctors sometimes refer to a stroke as a “brain attack.”
Technically speaking, a stroke occurs when some form of interruption to the brain’s blood supply causes damage to a portion of the brain. In some cases, this damage can be fatal. In other cases, it can cause long-term disability.
Strokes demonstrate the relationship between our brains and the rest of our bodies—especially our hearts. To work properly, our brains need oxygen. Nearly 400 miles of blood vessels deliver oxygen-rich blood to all parts of our brains. Dr. Stephen Cramer, a stroke neurologist at UCLA Health in Los Angeles, said that when a stroke happens, some part of the brain isn’t getting the minute-to-minute supplies it needs to continue operating.
“When the brain isn’t getting the supplies it needs, cells die,” Dr. Cramer told BrainWise. “Skin cells grow back, gut cells grow back, but brain cells don’t grow back. This can be a big challenge, depending on how many cells you lose.”
Depending on the type of stroke, scientists believe up to 1.2 million brain cells can die per minute—necessitating a quick response.
Quite literally, when it comes to treating strokes, every minute counts.
Two kinds of strokes
All told, there are nearly 800,000 strokes in America each year, according to the US Centers for Disease Control and Prevention. There are two main kinds of strokes: ischemic and hemorrhagic.
The former is essentially the result of a blocked artery; the latter the result of a ruptured one.
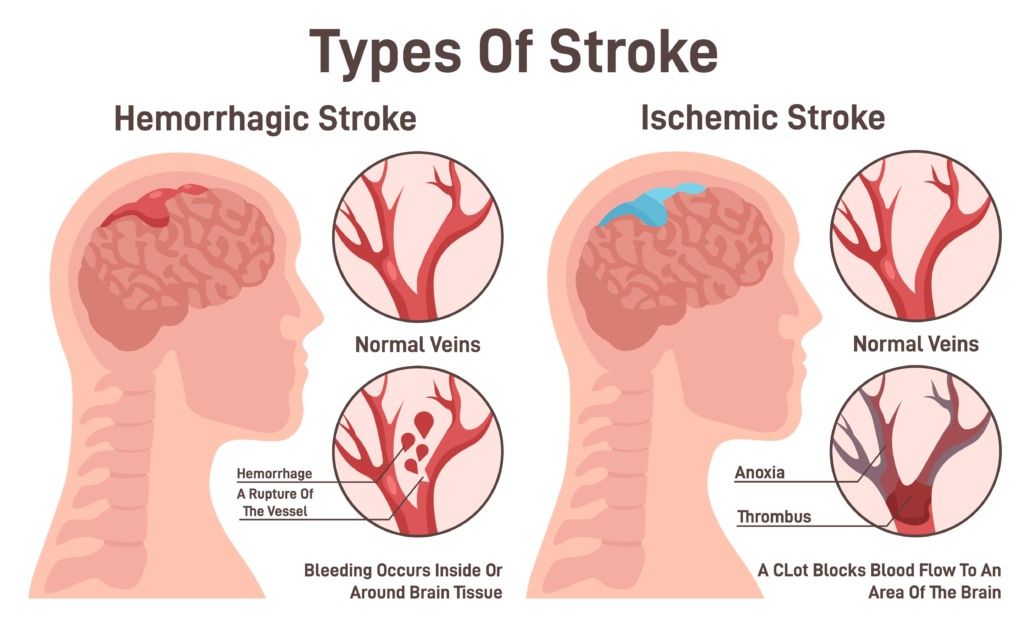
Ischemic strokes comprise nearly 85 percent of all strokes. An ischemic stroke occurs when blood clots or other particles block the blood vessels to the brain. Fatty deposits called plaque can also cause blockages by building up in the blood vessels.
This is precisely why it’s so important to stay healthy and manage telltale indicators such as cholesterol.
Dr. Thomas Hemmen, a vascular neurologist and director of the Stroke Center at UC San Diego Health, said that if a clot becomes dislodged from an artery elsewhere in the body, there’s no telling where it may end up getting stuck.
“It’s a bit like pinball,” he said. “This is what makes it so dangerous.”
Hemorrhagic strokes comprise the other roughly 15 percent of strokes. A hemorrhagic stroke happens when an artery in the brain leaks blood or breaks open and spurts blood everywhere (inside the brain). The leaked blood can damage brain cells in multiple ways.
According to Dr. Cramer, roughly 67 percent of hemorrhagic strokes occur in a blood vessel inside the brain—doctors call that an intracerebral hemorrhage.
Dr. Cramer said the other 33 percent of the time hemorrhagic strokes occur in the bigger blood vessels that run along the surface of the brain.
Causes of hemorrhagic strokes are varied. High blood pressure and aneurysms—balloon-like bulges in an artery that can stretch and burst—are examples of conditions that can cause a hemorrhagic stroke. Another potential cause: protein deposits in blood vessel walls that can lead to weakness in the vessels. This condition is known as cerebral amyloid angiopathy. Hemorrhages can also occur because of head injury, though these injury-related hemorrhages are not considered to be strokes.
A third kind of cerebrovascular incident, dubbed a Transient Ischemic Attack, or TIA, is considered to be a “mini stroke.” TIAs are also caused by blockages. The American Stroke Association says the main difference with a TIA is that it only lasts anywhere from five minutes to 24 hours, whereas other strokes can last for much longer. The clot in a TIA usually dissolves on its own or becomes dislodged.
Signs of stroke
Though strokes themselves can differ by happening in just about any part of the brain, certain symptoms can help us identify a large percentage of strokes quickly. According to the CDC, these are the five most common indicators that a patient might be experiencing a stroke:
- Sudden numbness or weakness in the face, arm, or leg, especially on one side of the body.
- Sudden confusion, trouble speaking, or difficulty understanding speech.
- Sudden trouble seeing in one or both eyes.
- Sudden trouble walking, dizziness, loss of balance, or lack of coordination.
- Sudden severe headache with no known cause.
Patients who experience any of these symptoms are encouraged to call 911 immediately so they can get treatment because time is critical in stroke treatment. Doctors must work fast to determine what’s going on. Dr. Cramer said this process often feels like a Herculean undertaking, at least until the first brain scans are taken.
“Being a stroke doc is like being ‘Columbo,’” he said. “You show up at the scene and there [are] no suspects; just a few clues to help you figure out what happened with a patch of dead brain. Was it the heart? Was it the big pipes? You have to find out.”
There is good news—doctors’ ability to intervene and facilitate recovery after a stroke is stronger than ever. More good news: Stroke patients who receive care quickly can recover well. Stroke victims who arrive at the emergency room and receive treatment within the first three to four hours of their first symptoms often have less disability three months after a stroke than those who received delayed care.
Of course, depending on the size of the stroke, the kind of stroke, and where in the brain a stroke occurs, the impact of that stroke may be different.
Dr. Hemmen said this is often one of the most difficult aspects of strokes to understand.
“If you get a blood clot in your lung, it’s terrible, but each part of the lung does the same thing, so you can lose a chunk and still live an OK life,” he said. “If you lose the chunk of your brain that controls your dominant hand, even with rehab, that can be devastating.”
Behind the numbers
The official data around strokes is startling. According to the CDC, someone dies from a stroke every 3 minutes and 14 seconds. In 2021, about one in six deaths from cardiovascular disease were due to stroke, and the death rate for stroke increased to 41.1 per 100,000 in 2021 from 38.8 per 100,000 in 2020. Stroke remains a leading cause of long-term disability for seniors in America.
Stroke risk increases with age, but just about anyone can have a stroke. In 2014—the last year for which data was available on this point—roughly 38 percent of people hospitalized for stroke were less than 38 years old.
A deeper look into some of the data suggests that while strokes are a leading cause of death for all Americans, the risk of having a stroke varies with race and ethnicity.
What’s more, about 610,000 of the nearly 800,000 people to have a stroke each year are having one for the first time. That means roughly 185,000 stroke victims are people who already have had a stroke at least once.
Staggering numbers extend to TIAs, too. More than a third of people who have a TIA and don’t get treatment have a major stroke within 1 year. As many as 10 to 15 percent of people will have a major stroke within 3 months of a TIA.
Fortunately, not all the data is negative.
According to Dr. Hemmen, current research suggests that one in three people who receive medicine to treat an ischemic stroke experience complete or near complete resolution of their stroke symptoms.
The future of stroke research
Stroke intervention has come a long way in the last few decades—in the past, having a stroke almost guaranteed disability or death; today, people can have strokes and make nearly complete recoveries.
At the same time, researchers are looking to the future to extend and amplify some of the strides they have made.
For starters, several studies are currently underway to evaluate the efficacy of new drugs that could push the critical response time to 24 from 4.5 hours. In addition, several teams of researchers are experimenting with how AI can assist doctors by reading brain scans for lesser-known or hard-to-find medical conditions.
According to several experts, robotics could help with acute stroke response, as well. Dr. Hemmen, the neurologist at UCSD, said this is a key movement right now because there simply aren’t enough medical teams to respond to the 800,000 strokes in America every year. Dr. Hemmen notes that robots likely won’t do procedures themselves, but instead will assist with catheter-based treatments and surgeries so doctors can do more of them, faster.
“Once we introduce this technology into the mix, we can broaden the response,” he said. “Anything that can improve our response to strokes is a step in the right direction.”
Other researchers are making strides in stroke rehabilitation—a practice that, at least in the United States, is not as prevalent as it is in other countries. Dr. Cramer, for instance, runs a lab that specializes in tele-rehab, essentially a way for patients to help those brain cells that remain after a stroke build new connections to make the patient’s brain stronger.
Currently, Dr. Cramer’s lab is focused on rehabbing arm movement; recovering stroke patients engage in activity-based therapy to re-learn how to use their arms.
Most of the therapy is in the form of games such as video poker and duck hunter; patients play these games online from the confines of their own homes.
“We’ve learned that the brain after a stroke is not just going to rewire out of nowhere,” Dr. Cramer said. “That’s why activity-based therapy is so [promising]. The more you do something, the better you’ll get.”
This article has been factchecked. For more about that process, click here.







